
Home
/
Recent Cases

From Injury Treatment to Insurance Claims: Care That Puts Patients First

How a Trauma Treatment Center Supports Recovery from Auto Injuries

Getting Proper Care for a Car Crash Injury Without the Insurance Stress

Car Accident Injury Treatment: How the Right Medical Care Supports Faster Healing

How Chiropractic Adjustment Helps Relieve Car Crash Injury Pain: A Scientific Path to Recovery

What Toxins Are Released After a Chiropractic Adjustment? Facts vs Myths

What to Expect from an Injury Rehabilitation Clinic During Your Recovery
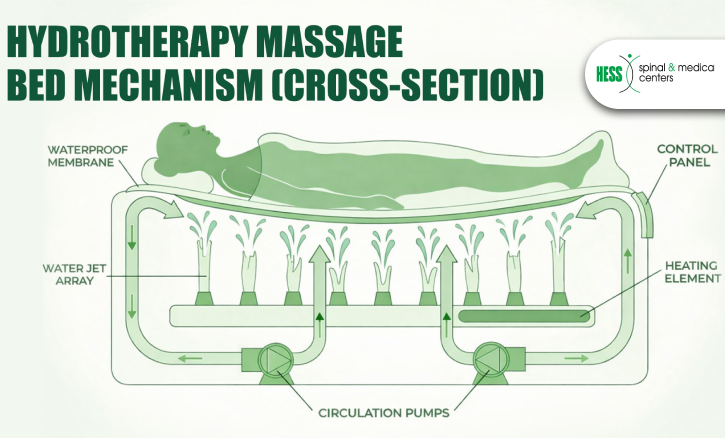
The Benefits of Hydrotherapy Massage for Auto Injury and Muscle Recovery

What Lifestyle Changes Can Support Your Chiropractic Treatment Results?

What’s the Real Difference Between a Chiropractic Adjustment and a Massage?